
There’s been a recent update to the Ministry of Health’s Virtual Care Program (previously called the Telemedicine Program).
Telemedicine was originally introduced as a way to treat remote patients, or in remote areas that lacked physicians. Nowadays, it’s becoming a more convenient type of medical care; it means less waiting time for patients and a more efficient way to quickly clear up minor, but not urgent, conditions.
Therefore, the Ontario Medical Association (OMA) and OHIP have decided it’s time to modernize and improve Ontario’s approach to virtual care. While this is an on-going project, they have recently implemented two major changes:
- Enabling Direct-to-Patient Video Visits so that patients can receive a video visit from their location of choice (e.g. in their home on their own device).
- Modernizing Virtual Care Compensation to reflect the maturation of virtual care technology and to align with compensation for in-person care.
1. Enabling Direct-to-Patient Telemedicine Video Visits
There are two types of video visits that you can use to speak with patients, a hosted video visit or, the newly introduced direct-to-patient video visit.
Hosted Video
A Hosted Video Visit is when you speak with a patient who is currently at a patient host site. A patient host site is an organization that provides patients with an on-site location with videoconferencing technology and, in some cases, clinical support services (nursing support, diagnostics through peripheral devices).
Since a hosted Video Visit is limited (as it still requires your patient to go to an organization) OMA and OHIP have recently introduced direct-to-patient video.
Direct-to-patient Video
A direct-to-patient video visit is when you speak with a patient who is either at their home or any other location besides a patient host site. This includes situations where your patient schedules and manages the encounter independently using their own technology, or where an organization provides support resources (e.g. access to technology).
In order to be eligible for payment for direct-to-patient telemedicine video visits, you need to register with the ministry’s Virtual Care Program. To register fill out the OHIP Virtual Care Physician & Dentist Registration Form and email it to serviceactivation@otn.ca or fax to 416-354-8280. Membership is free if you receive 50% or more of your earnings from OHIP.
Keep in mind, you’re only eligible for direct-to-patient telemedicine video if you are:
- A specialist;
- A GP physician has been designation by the OMA-Ministry GP Focused Practice Review Committee;
- A primary care physician that is in a patient enrolment model (PEM) and you’re delivering care to a rostered patient.
Medical billing in Ontario is confusing and can often be overwhelming. To help out, check out the Ultimate OHIP Billing Guide that walks you through each step of medical billing – from the general submission process to maximizing your claims and mobile billing.
General Requirements for all Telemedicine Video Visits
(hosted video and direct-to-patient video visit)
Whether you have a hosted video visit or a direct-to-patient video visit you must meet the following general requirements for video visits:
- Be registered with OTN,
- Be physically located within Ontario during the call,
- You and your patient must be present the whole time during the call in an approved OTN video solution,
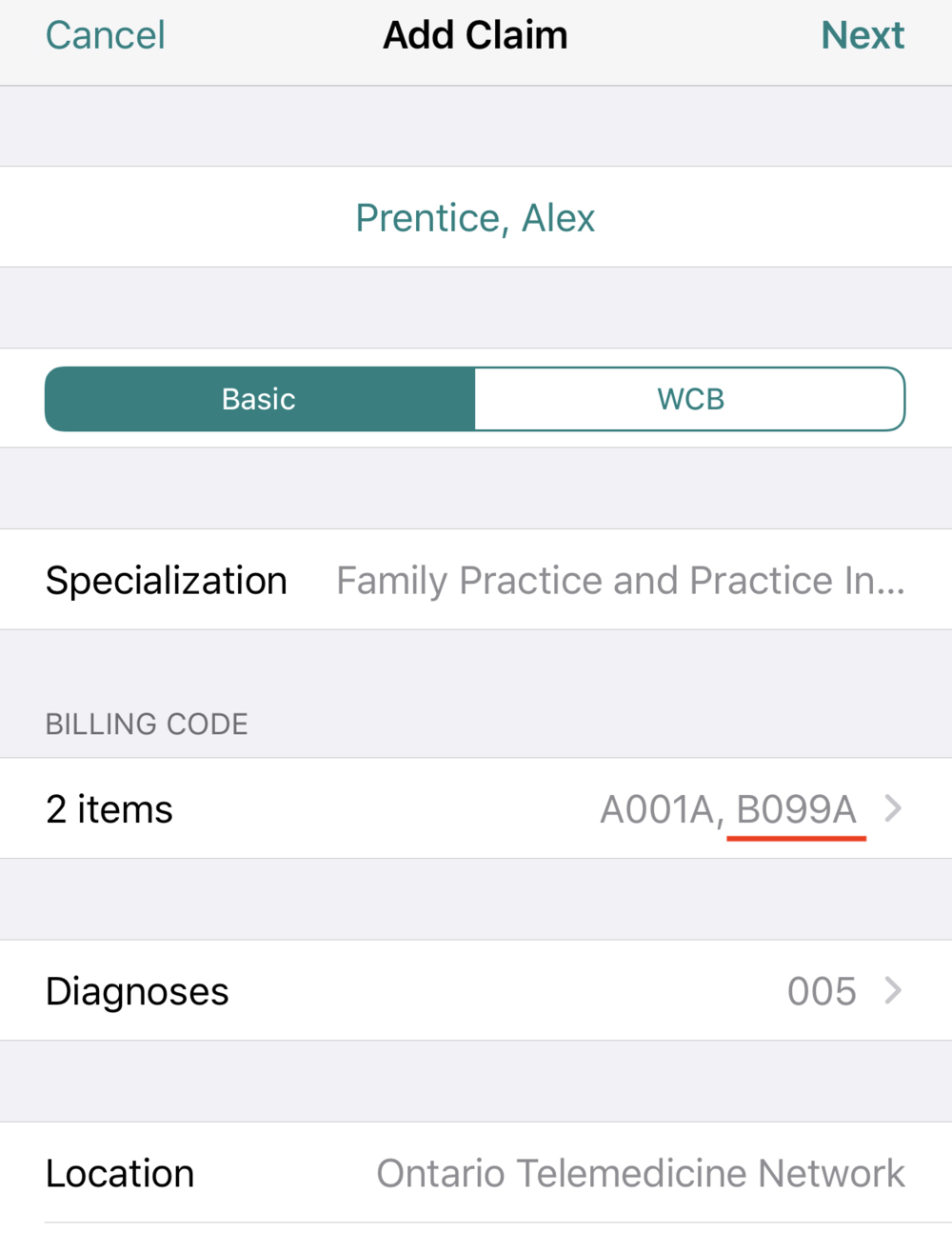
- Set the location (SLI) of your claim to ‘Ontario Telemedicine Network.’
- Select a billing code along with the applicable Virtual Care Program B-code (e.g. B099A, B100A, B200A); and
- Do not include fee codes for services excluded from the Virtual Care Program (see list below ‘excluded fee codes’).
Requirements for Hosted Video Visits
There are no additional requirements for Hosted Video Visits beyond the general requirements for all Video Visits provided above.
Requirements for Direct-to-Patient Video Visits
In addition to the general requirements above, to be eligible to bill direct-to-patient video visits you must also meet the following requirements:
- For Video Visits to be delivered they must be deemed to be appropriate according to your professional judgement and in the best interest of their patient [See CPSO telemedicine policy].
- Your patient must consent to receive a video visit.
Additional GP Focused Practice Designated Telemedicine Requirements:
- You have to have been designated by the OMA-Ministry GP Focused Practice Review Committee;
- You must be providing the video services within the scope of your designation (e.g. addiction medicine, pain management).
- You cannot provide Direct-to-Patient Video Visits for routine primary care.
Addition
al Primary Care Direct-to-Patient Video Visits
At this time you’re only eligible to bill direct-to-patient video visits in primary care if:
- You’re in a patient enrolment model (PEM);
- You’re delivering care to a patient rostered to the same PEM practice.
This means that any rostered patient in a PEM can see any physician in the PEM they are rostered to by a Direct-to-Patient Video Visit.
All PEM types are eligible. This includes Family Health Organization, Family Health Network, Family Health Group, Comprehensive Care Model, Blended Salary Model, Rural and Northern Physician Group Agreement, St. Joseph’s Health Centre, Weeneebayko Area Health Authority, GP Care of the Elderly, and GP HIV patient enrolment models.
Direct-to-Patient Video Visits for primary-care physicians who are not enrolled in PEM will be available in 2020. Expect more information between June-September of next year.
2. Telemedicine Virtual Care Compensation
The following fee codes are eligible for payment from November 15, 2019 – March 31, 2020:
Direct-to-Patient Video Visit:
B099A: $0.00 Tracking Code
You need to add a fee code and then the tacking code (B099A) to your claim. This aligns your compensation with in-person care since you’ll be compensated for the same amount whether you see your patient in-person or on video. It also let’s OHIP know it’s a direct-to-patient video visit.
Hosted Video Visit:
B100A: $35.00 First Telemedicine Patient
B200A: $15.00 Subsequent Telemedicine Patient
B101A: $35.00 First Cancelled/Missed Telemedicine Patient
B201A: $15.00 Subsequent Missed/Cancelled Telemedicine Patient
B102A: $35.00 First Technical Difficulties Abandoned Patient
B202A: $15.00 Subsequent Technical Difficulties Abandoned premium
***More Virtual Care Program codes will be released on April 1, 2020.
Telemedicine Premiums Removed
Telemedicine premiums were first introduced over 10 years ago when you were required to travel to an OTN telemedicine studio in order to conduct a video visit. However, since now you can easily access telemedicine visits from the comfort of your office – or even your smartphone – the need for telemedicine premiums are no longer needed.
Therefor, telemedicine premiums are slowly being phased out. Below are the current conditions when telemedicine premiums still apply:
-
In Transition
If you can demonstrate that there will be a significant negative impact to patient access to care due to impacts of the premium removal on your existing virtual care service, you can send feedback to OMA from November 15, 2019 to January 17, 2020.
This feedback will then go to the Virtual Care Working Group (created earlier this year between the Ministry, the OMA, OntarioMD and OTN) and they will further explore expansion of virtual care in Ontario.
-
Hosted Video Visits:
If you’re using Hosted Video Visits because your patient lives in a rural area then you’ll continue to get a $15 premium per completed video until March 31st, 2021.
Remember that rural patients are identified as patients living in communities with a Rurality Index of Ontario score of >=45.
-
Rural Physicians
If you’re a rural physician based on the OMA’s RIO Postal code lookup then for now your premiums will remain the same. Except changes sometime in 2020.
Excluded Telemedicine Services Fee Codes
The following OHIP Fee codes aren’t eligible for telemedicine:
1. Surgical services with a fee code prefix of D, E, (Except E078 and E079), F, M, N, P (Except P003, P004 and P005), R, S, and T and ending with an A or C suffix.
2. All J and Y prefixed fee codes with A, B or C suffixes (J***A, J***B, J***C, Y***A, Y***B, Y***C).
3. K050A, K051A, K052A, K053A, K054A, K055A, K065A, K066A, K053, K061, K623, K624, K629, K035, K036, K038, K027, K031, K070, K620.
4. All laboratory fee codes with a prefix of “L” (L***). These codes should only be billed by physicians for services performed for their own patients in their own offices. These codes are eligible for payment through OHIP, not telemedicine.
5. All X prefixed fee codes with B or C suffixes (X***B, X***C).
G491A: Thermography – 1 or more area – prof
G505A: Phonocardiogram-mult. chan.-tech
G506A: Phonocardiogram w/pharmac.int.
G508A: Apex cardiogram-tech. component
G519A: Phlebography and/or carotid pulse tracing (with systolic time intervals) – technical component
G538A: Other immunizing agents not listed above
G540A: Technical component … per unit
G542A: Technical component
G544A: Technical component, per item … add
G554A: Technical component
G560A: Phonocardiogram w/pharmac.int.
G566A: Echocardiogram. comple.-2 dim. tech
G570A: Complete Study – 1 and 2 dimensions – technical component
G574A: Focused Study – not to be claimed in conjunction with pregnancy study – technical component.
G577A: Card. drop.-compl. 1&2-echo-tech.
G590A: Influenza agent
G651A: Level 1 – technical component 12 to 35 hours recording
G652A: Level 1 – technical component 12 to 35 hours scanning
G654A: Level 2 – technical component 12 to 35 hours recording
G655A: Level 2 – technical component 12 to 35 hours scanning
G661A: Event recorder – technical component
G682A: Level 1 – technical co
mponent 36 to 59 hours recording
G683A: Level 1 – technical component 36 to 59 hours scanning
G684A: Level 1 – technical component 60 hours to 13 days recording
G685A: Level 1 – technical component 60 hours to 13 days scanning
G686A: Level 2 – technical component 36 to 59 hours recording
G687A: Level 2 – technical component 36 to 59 hours scanning
G688A: Level 2 – technical component 60 hours to 13 days recording
G689A: Level 2 – technical component 60 hours to 13 days scanning
G692A: Cardiac loop monitoring (per 14 day test) – technical component
G693A: no description
G815A: Electrocochleography (per ear): to include myringotomy if performed – technical component
G850A: Colour vision detailed assessment – technical component
G851A: Dark adaptation curve (Goldmann adaptometer or equivalent) – technical component
G852A: Electro-retinography with report – Full field or multi-focal electro-retinography – technical component
G853A: Fluorescein angiography – technical component
G854A: Fluorescein angioscopy – technical component
G855A: Hess screen examination – technical component
G856A: Tonography (to include tonometry) with or without water – technical component
G857A: Visual fields – kinetic (with permanent record) – technical component
G858A: Visual fields – static – technical component
6. The following fee codes:
G104A: Positional testing with electronystagmography (ENG) – technical component
G111A: Dipyramidole Thallium stress test – technical component
G121A: Impedance plethysmography – technical component
G140A: Upper or lower limbs – technical component
G143A: Cortical evoked audiometry – technical component
G146A: Brain stem evoked audiometry – technical component
G149A: Visual evoked response – simple – technical component
G152A: Visual evoked response – threshold – technical component
G153: Cortical evoked audiometry, multiple frequency (minimum of 4 frequencies in each ear).
G154: Cortical evoked audiometry multiple frequency (minimum of 4 frequencies in each ear) WSIB.
G167A: Hydrogen breath test – technical component
G174A: Dobutamine stress test – technical component, when rendered outside of hospital … add
G181A: Dual chamber reprogramming including electrocardiography – technical component
G209A: Skin testing – technical component, to a maximum of 50 per year … per test
G284A: Single chamber reprogramming including electrocardiography – technical component
G308: Pacemaker pulse wave analysis including electrocardiography – technical component
G310A: Electrocardiogram – twelve lead – technical component
G311A: Interpretation of telephone transmitted ECG rhythm strip – technical component
G315A: Maximal stress ECG – technical component
G316A,
G372A: with visit (each injection)
G373A: – sole reason (first injection)
G414A: Routine EEG – technical component
G416A: EEG with activating/sleep inducing drugs
G434A: Manuel impedance testing-tech
G440A: Pure tone threshold audiometry with or without bone conduction – technical component
G441A: Pure tone threshold audiometry (with or without bone conduction) and speech reception threshold and/or speech discrimination scores. – technical component
G442A: Impedance audiometry by manual or automated methods – technical component
G443A: Miscellaneous advanced testing e.g. recruitment, tests of malingering, central auditory and stapedial reflex decay tests – per test – technical component, to a maximum of 1 … per test
G445A: Hear, aid re-evaluati.-tech company
G448A: Sound field audiometry (infants and children) – technical component
G451A: Caloric testing with ENG – technical component
G455A: Schedule A – technical component
G466A:
In Closing…
Over the next year, the ministry, in partnership with the OMA, will be looking at expanding virtual care to include electronic secure messaging and a wider range of options than what is currently being offered through the Ontario Telemedicine Network (OTN) program. Stay tuned!
This article offers general information only and is not intended as legal, financial or other professional advice. A professional advisor should be consulted regarding your specific situation. While information presented is believed to be factual and current, its accuracy is not guaranteed and it should not be regarded as a complete analysis of the subjects discussed. All expressions of opinion reflect the judgment of the author(s) as of the date of publication and are subject to change. No endorsement of any third parties or their advice, opinions, information, products or services is expressly given or implied by RBC Ventures Inc. or its affiliates.
Add Claims in Seconds
Our software helps you save time, collaborate with ease and get expert support.




